
The Ultimate Guide to Hospital Medical Equipment Planning and Equipment Lists
Table of Contents
- What Is Hospital Medical Equipment Planning?
- Why Hospital Medical Equipment Planning Is Critical in Modern Healthcare
- The Biomedical Engineer’s Role in Hospital Equipment Planning
- The Complete 7-Step Hospital Medical Equipment Planning Process
- 4.1 Step 1: Define Clinical Services and Care Model
- 4.2 Step 2: Department-Level Equipment Needs Assessment
- 4.3 Step 3: Develop the Medical Equipment List (MEL)
- 4.4 Step 4: Infrastructure & Interface Coordination
- 4.5 Step 5: Budgeting and Lifecycle Cost Analysis
- 4.6 Step 6: Technical Specifications & Procurement Support
- 4.7 Step 7: Installation Planning and Commissioning Readiness
- How to Create a Hospital Medical Equipment List (MEL)
- 5.1 Core Components of an MEL
- 5.2 Risk Classification and Criticality Levels
- 5.3 Infrastructure Requirement Mapping
- Department-Specific Equipment Planning Examples
- 6.1 ICU Equipment Planning
- 6.2 Operating Room Equipment Planning
- 6.3 Imaging Department Equipment Planning
- 6.4 Emergency Department Equipment Planning
- Hospital Equipment Budgeting and Lifecycle Costing
- 7.1 Capital vs Operational Costs
- 7.2 Service Contracts and Spare Parts Planning
- 7.3 Obsolescence and Replacement Strategy
- Standards and Regulations Relevant to Equipment Planning
- 8.1 Electrical Safety and IEC 60601
- 8.2 Risk Management and ISO 14971
- 8.3 WHO and Healthcare Technology Management Guidance
- Common Failures in Hospital Equipment Planning Projects
- Career Pathways in Medical Equipment Planning and Healthcare Projects
- Frequently Asked Questions (FAQ)
- References
What Is Hospital Medical Equipment Planning?
Hospital medical equipment planning is the structured engineering process used to define, specify, budget, and integrate medical devices into a healthcare facility in a safe, compliant, and operationally sustainable way.
From a biomedical engineering perspective, it is not simply “creating a hospital equipment list.” It is:
A systems-engineering discipline that aligns clinical services, building infrastructure, risk management, lifecycle costs, and regulatory compliance into one coordinated technology framework.
This process is essential in:
- New hospital construction
- Hospital expansion projects
- ICU or OR upgrades
- Imaging department installation
- National healthcare infrastructure programs
Biomedical engineers are the technical architects of this system.
What You Will Learn
By the end of this guide, you will understand:
- The full 7-step hospital medical equipment planning process
- How to create and validate a Medical Equipment List (MEL)
- How biomedical engineers coordinate with architects and MEP engineers
- How budgeting and lifecycle costing influence planning
- What standards and guidelines apply
- Common mistakes that cause multimillion-dollar hospital failures
This article is written specifically for biomedical engineers, not clinicians or general audiences.
Why Hospital Medical Equipment Planning Exists
Modern hospitals are technology-dependent ecosystems.
An ICU cannot function without:
- Ventilators
- Monitoring systems
- Infusion pumps
- Defibrillators
An operating room requires:
- Anesthesia workstations
- Surgical lights
- Electrosurgical units
- Imaging systems
- Integrated power and gas systems
If equipment planning is done incorrectly:
- Devices may not match electrical capacity
- Medical gas outlets may be insufficient
- IT networks may be overloaded
- Safety clearances may be violated
- Maintenance may become unsustainable
The cost of poor equipment planning is not theoretical — it results in:
- Delayed hospital openings
- Regulatory non-compliance
- Increased clinical risk
- Budget overruns
- Long-term operational inefficiency
This is why hospital equipment planning is a formal engineering discipline, not an administrative task.
The 7-Step Hospital Medical Equipment Planning Process
Below is the complete, real-world workflow used in professional hospital projects.
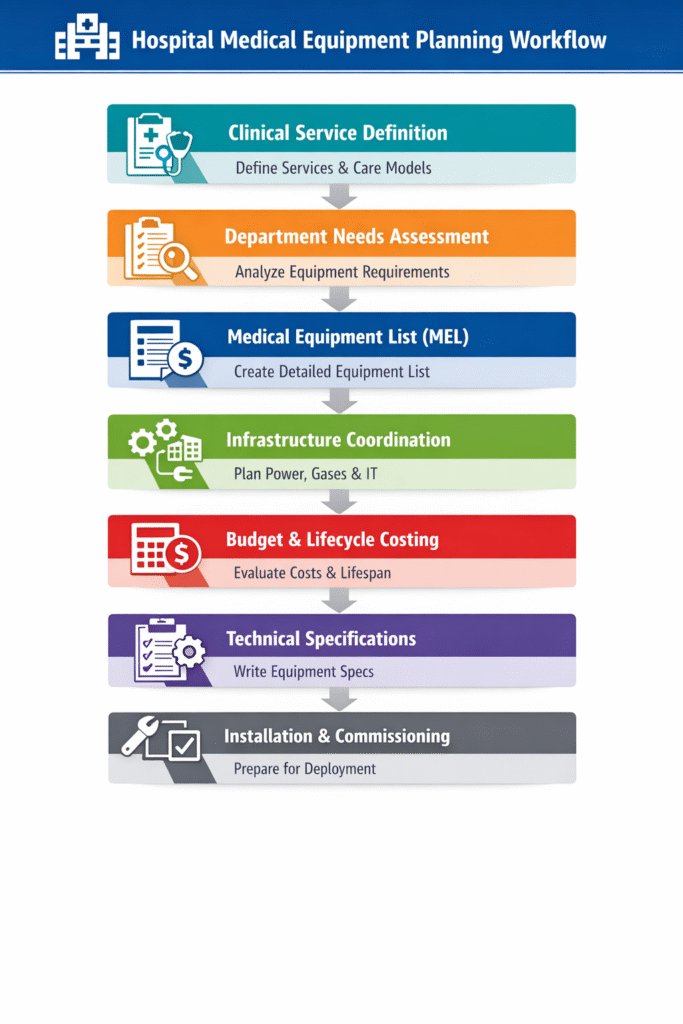
Step 1: Define Clinical Services and Care Model
Before listing devices, biomedical engineers must understand:
- What specialties will operate?
- What is the expected patient volume?
- What level of acuity (secondary, tertiary, trauma)?
- What is the model of care (centralized ICU, modular ORs, hybrid rooms)?
This phase answers:
What must this hospital be capable of delivering?
Without this step, device lists become arbitrary and disconnected from clinical reality.
Step 2: Department-Level Equipment Needs Assessment
For each department (ICU, OR, Imaging, Emergency), biomedical engineers conduct structured sessions with clinicians.
The objective is to define:
- Functional requirements (not brand names)
- Quantity ranges
- Redundancy levels
- Critical vs non-critical equipment
- Interoperability requirements
Example: ICU Equipment Planning List (High-Level)
| Category | Examples | Planning Considerations |
|---|---|---|
| Life Support | Ventilators | Redundancy, gas supply capacity |
| Monitoring | Multiparameter monitors | Central station integration |
| Infusion | Syringe/volumetric pumps | Electrical load distribution |
| Emergency | Defibrillators | Strategic placement |
| Diagnostics | Portable ultrasound | Mobility and storage |
The biomedical engineer ensures this list is:
- Clinically sufficient
- Technically feasible
- Infrastructure-compatible
Step 3: Development of the Medical Equipment List (MEL)
The Medical Equipment List (MEL) is the core planning document.
It typically includes:
- Equipment category
- Functional description
- Department/location
- Quantity
- Risk classification
- Power requirements
- Medical gas requirements
- Data/network needs
- Preliminary cost estimate
This document becomes the foundation for:
- Infrastructure design
- Budgeting
- Tender preparation
- Project management
A poorly developed MEL leads to systemic project failure.
Step 4: Infrastructure & Interface Coordination
Medical devices interact with hospital building systems:
Electrical Systems
- Normal power
- Essential power (generator-backed)
- UPS lines
- Load calculations
Medical Gases
- Oxygen
- Medical air
- Vacuum
- Nitrous oxide (where applicable)
HVAC
- Temperature and humidity control
- Air changes per hour (critical in ORs)
IT & Networking
- PACS integration
- EMR compatibility
- Cybersecurity protocols
Biomedical engineers coordinate with:
- Electrical engineers
- Mechanical engineers
- IT architects
- Structural engineers
This phase prevents:
- Insufficient power outlets
- Inadequate shielding for imaging
- Improper gas pipeline sizing
- Network bottlenecks
Step 5: Budgeting and Lifecycle Cost Analysis
One of the most misunderstood aspects of hospital medical equipment planning is lifecycle costing.
Purchase price represents only part of the cost.
Biomedical engineers evaluate:
- Installation and site preparation
- Service contracts
- Spare parts
- Consumables
- Calibration costs
- Expected lifespan
- Decommissioning costs
Lifecycle thinking aligns with international healthcare technology management guidance from organizations such as the World Health Organization (WHO) and best practices outlined in clinical engineering literature.
Without lifecycle analysis, hospitals risk:
- Underfunded maintenance
- Excessive downtime
- Early equipment obsolescence
Step 6: Technical Specifications & Procurement Support
Once planning is approved, biomedical engineers:
- Develop detailed technical specifications
- Ensure compliance with IEC 60601 safety standards
- Verify regulatory approvals (e.g., CE marking or FDA clearance)
- Participate in technical bid evaluation
- Review service contract conditions
This ensures procurement aligns with:
- Safety standards
- Clinical needs
- Infrastructure compatibility
- Long-term serviceability
Step 7: Installation Planning & Commissioning Readiness
Even before procurement is finalized, biomedical engineers plan for:
- Equipment delivery logistics
- Storage requirements
- Installation sequence
- Acceptance testing procedures
- Staff training coordination
Commissioning includes:
- Electrical safety testing (per IEC frameworks)
- Functional performance verification
- Integration testing
- Documentation review
Only after these steps is equipment released for clinical use.
Common Mistakes in Hospital Equipment Planning
- Creating device lists without infrastructure coordination
- Selecting equipment based only on lowest price
- Ignoring maintenance capacity
- Failing to classify critical vs non-critical equipment
- Overlooking IT and cybersecurity integration
- Underestimating consumable costs
- Planning too late in the construction timeline
These failures often result in project delays and cost escalation.
Standards and Guidance Relevant to Equipment Planning
Hospital equipment planning aligns with frameworks such as:
- IEC 60601 series (Medical electrical equipment safety)
- ISO 14971 (Risk management for medical devices)
- WHO medical device technical guidance
- AAMI clinical engineering guidance
- National hospital construction regulations
Biomedical engineers interpret and apply these standards within the hospital context.
The Biomedical Engineer’s Unique Value in Equipment Planning
Biomedical engineers uniquely combine:
- Clinical understanding
- Engineering systems analysis
- Risk management
- Regulatory awareness
- Lifecycle thinking
They serve as:
- Translators between clinicians and engineers
- Risk mitigators
- Infrastructure integrators
- Technology strategists
No other hospital professional occupies this intersection.
Career Pathways in Hospital Equipment Planning
Professionals in this domain may work as:
- Hospital Biomedical Engineers
- Clinical Engineers
- Healthcare Project Engineers
- Medical Equipment Planning Consultants
- Government Healthcare Infrastructure Advisors
This field often serves as a gateway to:
- Healthcare Technology Management (HTM)
- Hospital leadership roles
- Medical device industry transitions
- International healthcare development projects
Frequently Asked Questions (SEO Optimized)
What is a Medical Equipment List (MEL)?
A Medical Equipment List (MEL) is a structured document that details all planned medical devices in a hospital project, including quantities, infrastructure needs, and preliminary costs.
Who is responsible for hospital medical equipment planning?
Biomedical engineers or clinical engineers typically lead the technical aspects, collaborating with clinicians, architects, and hospital administrators.
When should equipment planning begin in a hospital project?
It should begin during early architectural design — not after construction starts.
How is ICU equipment planning different from general ward planning?
ICU planning involves higher-risk devices, redundancy requirements, essential power integration, and advanced monitoring systems.
References
- World Health Organization (WHO). Medical Device Technical Series: Medical Equipment Maintenance Programme Overview.
- WHO. Medical Equipment Planning Guidance Documents.
- IEC 60601 Series – Medical Electrical Equipment Standards.
- ISO 14971: Medical Devices — Application of Risk Management.
- AAMI. Clinical Engineering Handbook.
- ECRI Institute. Healthcare Technology Management guidance publications.

