
The Holter monitor is one of the most clinically important tools in cardiac diagnostics, enabling the continuous capture of a patient’s heart rhythm over 24 hours or more during normal daily activities. For biomedical engineers, the device represents a fascinating convergence of biopotential sensing, low-noise analog front-end design, embedded data storage, and digital signal processing — all packaged in a compact, patient-friendly form factor. This comprehensive overview covers its history, operating principles, component architecture, clinical variants, regulatory landscape, and the AI-driven innovations reshaping ambulatory cardiac monitoring today.
- What is a Holter Monitor?
- Why is the Holter Monitor Used?
- How Does a Holter Monitor Work?
- What are the Main Components of a Holter Monitor?
- What Types and Variants of Holter Monitors Exist?
- What are the Main Benefits of the Holter Monitor?
- What are the Risks and Limitations of the Holter Monitor?
- How is the Holter Monitor Evolving? Recent Innovations
- Key Takeaways and Tips for Biomedical Engineers
What is a Holter Monitor?
A Holter monitor is a portable, battery-powered electrocardiographic recording device designed to continuously capture the electrical activity of the heart over an extended period, typically 24 to 48 hours. Unlike a standard ECG machine, which records cardiac signals for only a few seconds in a clinical setting, the Holter monitor enables ambulatory monitoring, allowing patients to go about their daily routines while their cardiac rhythm is continuously logged for later analysis.
The device is named after its inventor, Norman J. Holter, an American biophysicist who first developed the concept of ambulatory electrocardiography in 1947. His original prototype was far from portable — it weighed approximately 85 pounds and was carried as a backpack, transmitting cardiac data via radio telemetry. Over subsequent decades, advances in miniaturized electronics and data storage technologies dramatically reduced the size and weight of the device. The first commercially viable Holter monitor was brought to market in 1962 by Del Mar Avionics, marking a pivotal milestone in non-invasive cardiac diagnostics.
For biomedical engineers, the Holter monitor represents a compelling intersection of analog signal acquisition, digital signal processing, electrode interface design, and compact embedded systems engineering. The device must reliably acquire low-amplitude biopotential signals (typically 0.5–5 mV for QRS complexes) in the presence of motion artifacts, electrical noise, and variable patient anatomy — engineering challenges that have driven decades of innovation in the field.
Today, Holter monitoring is a cornerstone of cardiology, with millions of studies performed annually worldwide. Modern systems integrate flash memory storage, wireless data transmission, and cloud-based AI analytics, reflecting the rapid convergence of medical device engineering and digital health technology. Understanding the Holter monitor’s design principles and clinical utility is essential knowledge for any biomedical engineer working in the cardiovascular diagnostic space.


Why is the Holter Monitor Used?
The Holter monitor is used primarily to detect and characterize cardiac arrhythmias and conduction abnormalities that occur intermittently and are therefore unlikely to be captured during a brief resting ECG. Many significant arrhythmias — including atrial fibrillation (AFib), ventricular tachycardia (VT), supraventricular tachycardia (SVT), heart block, and sick sinus syndrome — may be entirely asymptomatic at the time of a clinic visit, or may occur unpredictably in response to physical activity, emotional stress, or sleep.

Primary Clinical Indications
Clinicians prescribe Holter monitoring across a broad range of clinical scenarios. The most common indications include evaluation of unexplained palpitations, presyncope, and syncope. When a patient experiences episodes of dizziness or fainting without a clear structural cardiac cause identified on echocardiography or standard ECG, Holter recording provides a temporal correlation between symptoms and rhythm disturbances. A patient event button integrated into most devices allows the individual to mark the moment symptoms occur, enabling physicians to directly link subjective complaints to objective electrophysiological findings.
- Arrhythmia detection: Identification and quantification of AFib burden, premature ventricular contractions (PVCs), runs of VT, SVT episodes, and pause events.
- Syncope and presyncope workup: Determining whether loss of consciousness or near-fainting is of cardiac origin.
- Palpitation evaluation: Correlating patient-reported symptoms with rhythm data during normal daily activities.
- Post-procedure monitoring: Assessing rhythm stability following ablation procedures, cardiac surgery, or pacemaker implantation.
- Medication effectiveness: Monitoring the efficacy and proarrhythmic potential of antiarrhythmic drugs such as amiodarone, flecainide, or sotalol.
- Myocardial ischemia detection: Identifying ST-segment changes indicative of silent ischemia, particularly in diabetic or high-risk populations.
Engineering Relevance of Clinical Use Cases
Each clinical use case places specific demands on the device’s engineering design. Arrhythmia detection requires high-fidelity QRS complex capture and accurate R-R interval measurement, demanding sampling rates of at least 200 Hz (with 500–1000 Hz preferred for morphological analysis) and a frequency response of 0.05–150 Hz. Ischemia monitoring requires precise ST-segment amplitude resolution, necessitating an analog front-end with sub-microvolt noise floors and strict DC offset management. The event-marking function requires responsive user interface hardware with timestamp synchronization to the internal clock. These requirements collectively define the performance specifications that biomedical engineers must meet in Holter system design.
Beyond diagnosis, Holter data feeds into heart rate variability (HRV) analysis — a powerful non-invasive marker of autonomic nervous system function used in risk stratification for post-MI patients, heart failure management, and even sports medicine. The accurate extraction of R-R intervals from Holter recordings, with sub-millisecond temporal precision, is therefore critical to the downstream validity of HRV metrics.
How Does a Holter Monitor Work?
The operating principle of the Holter monitor is rooted in the same galvanometer-derived electrocardiographic principle that underlies all surface ECG recording. The heart’s electrical depolarization and repolarization waves generate biopotential signals that propagate through the body’s conductive tissues and fluids to the skin surface, where they can be detected as differential voltages between electrode pairs. The Holter system captures, amplifies, filters, digitizes, and stores these signals continuously for the duration of the monitoring period.
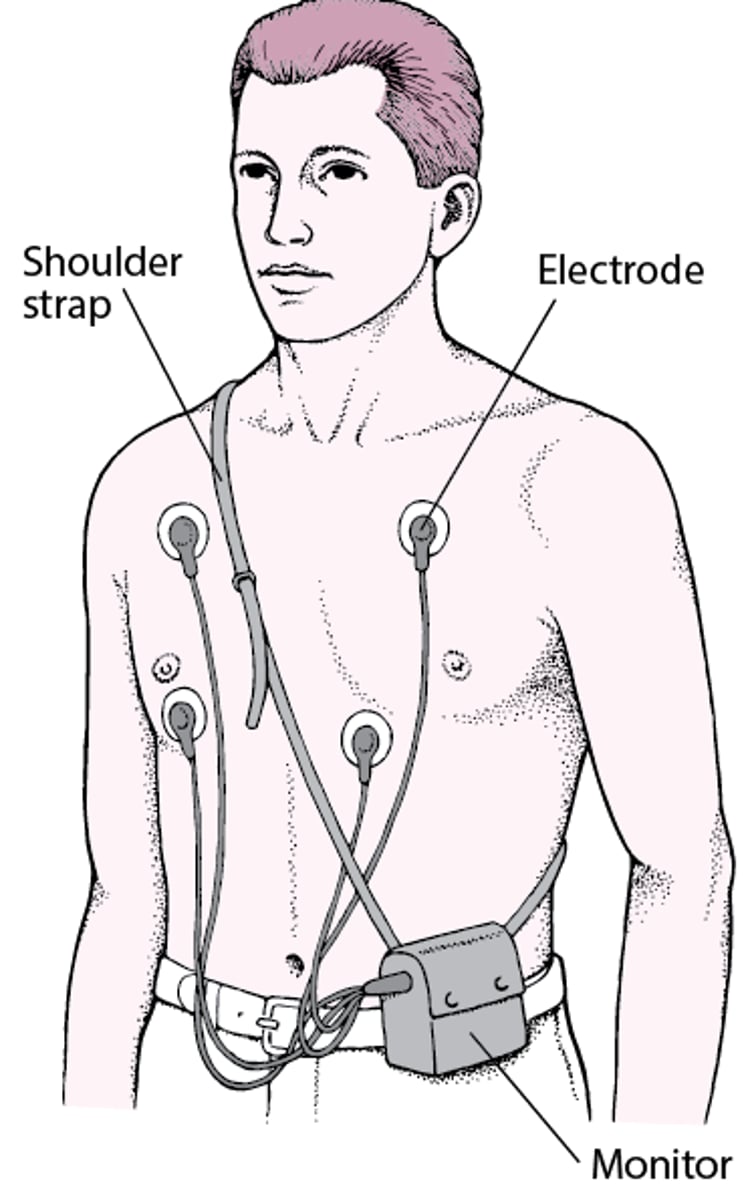
Signal Acquisition and Electrode Configuration
Holter monitors use between 3 and 8 chest electrodes, depending on the number of recording channels. Standard 2- to 3-channel systems employ modified bipolar lead configurations — such as modified limb leads (CM5, CM1, and a modified aVF equivalent) — strategically positioned on the torso to maximize sensitivity for different regions of the myocardium. Each electrode pair forms a lead, and the differential voltage across each lead is fed into a dedicated instrumentation amplifier channel. Proper skin preparation (abrasion and cleaning) is critical to minimize contact impedance, which should ideally be below 5 kΩ to ensure signal quality throughout the recording period.
The analog front-end applies a bandpass filter (typically 0.05–150 Hz) to remove DC offset and high-frequency noise before amplification. A driven right leg (DRL) circuit is commonly employed to actively reduce common-mode noise, particularly 50/60 Hz power line interference. The amplified signal is then digitized by an analog-to-digital converter (ADC), with modern systems operating at 500–1000 samples per second per channel and 12–16 bit resolution to faithfully represent both the gross morphology and fine temporal details of each cardiac cycle.

Data Storage and Retrieval
Early Holter monitors recorded onto magnetic tape cassettes at reduced speed — a technology that limited bandwidth and introduced speed-related artifacts during playback analysis. Contemporary devices utilize solid-state flash memory cards (SD or proprietary formats) capable of storing multiple days of multi-channel, high-resolution ECG data. A 48-hour, 3-channel recording at 500 Hz with 12-bit resolution generates approximately 500–600 MB of raw data, well within the capacity of modern flash storage. An integrated real-time clock (RTC) module timestamps every data sample, enabling precise correlation of rhythm findings with the patient’s activity diary and event markers.
Upon completion of the recording period, data is transferred to a Holter analysis workstation — either via physical media, USB, or wireless transmission — where automated detection algorithms identify P waves, QRS complexes, and T waves, measure intervals, and classify beats and rhythm episodes. Technicians and cardiologists then review the automated analysis, with final interpretation informing clinical decision-making. The accuracy of automated QRS detection directly impacts diagnostic yield, makin algorithm performance a critical biomedical engineering concern.
(1): Atrial fibrillation recorded by a Holter monitor.
(2): Screenshot of a computer software used to analyze Holter ECG recordings.


What are the Main Components of a Holter Monitor?
A complete Holter monitoring system consists of several interdependent hardware and software subsystems, each with distinct engineering specifications and performance requirements. Understanding the function and design constraints of each component is essential for biomedical engineers involved in device development, quality assurance, or clinical equipment management.
Electrodes and Lead Wires
Disposable Ag/AgCl (silver/silver chloride) snap electrodes are the industry standard for Holter recordings. Their electrochemical stability and low half-cell potential (~0.222 V) minimize DC offset and polarization artifacts, which is especially important during the extended recording periods characteristic of Holter studies. The electrode gel interface reduces skin-electrode impedance and maintains signal quality during patient movement. Lead wires connect the electrodes to the recorder via shielded, flexible cables designed to minimize triboelectric noise — a critical source of motion artifact. Lead wire strain relief and connector locking mechanisms must be robust enough to survive 24–48 hours of continuous patient activity without signal interruption.
Analog Front-End and Amplifier Circuitry
The recorder houses a precision instrumentation amplifier for each channel, featuring high input impedance (>10 MΩ), high common-mode rejection ratio (CMRR >90 dB), and very low input-referred noise (<1 µV RMS). These specifications ensure that the sub-millivolt P-wave and T-wave signals can be resolved even in the presence of electrode noise and patient movement artifacts. Programmable gain stages allow the system to accommodate the wide inter-patient variability in QRS amplitude, preventing both signal clipping and under-amplification. The DRL circuit actively injects a feedback signal to the body to suppress common-mode interference, particularly 50/60 Hz mains noise.
Microcontroller, ADC, and Storage
A low-power microcontroller unit (MCU) orchestrates all recorder functions: controlling ADC sampling, managing memory writes, processing event button inputs, and maintaining the real-time clock. Modern Holter recorders employ application-specific integrated circuits (ASICs) or system-on-chip (SoC) solutions that integrate the analog front-end, ADC, and digital processing in a single package, dramatically reducing board area and power consumption. Battery life is a critical design parameter; most recorders are powered by standard AA or AAA alkaline cells or lithium-ion batteries providing 48–72 hours of continuous operation.
- Electrodes: Disposable Ag/AgCl with conductive gel; 3–8 per patient setup.
- Instrumentation amplifiers: High CMRR, low-noise differential amplifiers for each channel.
- ADC: 12–16 bit resolution at 500–1000 Hz per channel.
- Flash memory: SD card or proprietary solid-state storage (2–32 GB).
- Real-time clock: Crystal-oscillator-based with ±1 ppm accuracy for precise timestamping.
- Patient event button: Debounced tactile switch with timestamp logging.
- Power supply: Battery pack with low-dropout regulator and power management IC.
- Analysis workstation: PC-based software for automated beat detection, arrhythmia classification, and report generation.
The analysis software represents a significant engineering component in its own right. Modern Holter analysis platforms employ machine learning algorithms — including convolutional neural networks (CNNs) trained on annotated databases such as MIT-BIH — to automate QRS detection, beat classification, and arrhythmia episode identification with sensitivities and specificities exceeding 98% for common arrhythmia types. This computational layer is as critical to the clinical utility of the Holter system as the hardware acquisition chain, and biomedical engineers increasingly contribute to both domains.
What Types and Variants of Holter Monitors Exist?
Since the introduction of the first commercial Holter monitor in 1962, the technology has diversified considerably to address the varying clinical needs of different patient populations and diagnostic scenarios. Today, the term “ambulatory cardiac monitoring” encompasses a spectrum of devices with different recording durations, channel counts, form factors, and transmission capabilities. Understanding this landscape is essential for biomedical engineers involved in device selection, procurement, or development.
Standard Holter Monitor (2–3 Channel)
The conventional Holter monitor records 2–3 ECG channels continuously over 24–48 hours using modified bipolar lead configurations. These devices remain the workhorse of outpatient arrhythmia diagnosis due to their relatively low cost, established clinical workflow, and sufficient diagnostic yield for frequent arrhythmias. Their primary limitation is the fixed recording window — if an arrhythmia does not occur during the monitoring period, it will not be captured.
12-Lead Holter Monitor
Devices such as the Mortara H12+ record all 12 standard ECG leads simultaneously over 24 hours, providing the full diagnostic information of a resting 12-lead ECG in an ambulatory format. This enables detailed ST-segment morphology analysis for ischemia assessment and precise arrhythmia localization — capabilities unavailable with standard 2–3 channel systems. The engineering trade-off is increased electrode count (10 electrodes), greater data volume, and higher patient burden. Similar to how a CT scanner provides volumetric imaging detail unavailable from a plain radiograph, the 12-lead Holter provides spatial ECG information unobtainable from a standard 2-channel device.
Extended-Wear Patch Monitors
Wearable patch monitors such as the iRhythm Zio Patch adhere directly to the chest skin as a single self-contained unit, eliminating lead wires and external recorders entirely. These devices can record continuously for up to 14 days on a single charge, dramatically increasing the probability of capturing infrequent arrhythmias. Data is stored internally and analysed after the patch is returned by the patient or mail. The engineering innovation lies in integrating dry electrodes, signal conditioning, storage, and battery into a thin, waterproof, skin-adhesive form factor — a significant challenge in flexible electronics and biocompatible materials engineering.
Mobile Cardiac Outpatient Telemetry (MCOT)
Systems such as CardioNet MCOT combine continuous ECG recording with real-time wireless transmission to a remote monitoring center via cellular networks. Onboard algorithms automatically detect potentially dangerous arrhythmias and transmit alerts within minutes, enabling same-day clinical intervention. This real-time telemetry capability represents a significant advance over store-and-forward Holter systems for high-risk patients and is increasingly supported by cloud-based AI triage platforms.
Implantable Loop Recorder (ILR)
For patients with very infrequent but high-impact symptoms such as unexplained syncope, the implantable loop recorder — exemplified by the Medtronic Reveal LINQ — offers monitoring durations of up to 3 years from a device implanted subcutaneously in the left parasternal region. At 1.2 mL volume, the Reveal LINQ is the world’s smallest cardiac monitor, representing the pinnacle of miniaturization in implantable biomedical device engineering. Remote data transmission via a home bedside communicator enables continuous physician oversight without clinic visits.
Comparative Overview of Holter Monitor Types
The table below summarizes the key technical and clinical characteristics of the major ambulatory cardiac monitoring device types, providing a concise reference for biomedical engineers evaluating these systems:
| Device Type | Recording Duration | Channels / Leads | Data Transmission | Key Advantage | Key Limitation | Example Device |
|---|---|---|---|---|---|---|
| Standard Holter | 24–48 hours | 2–3 channels | Store and forward | Low cost; established workflow | Short window; misses infrequent events | Spacelabs UltraView |
| 12-Lead Holter | 24–48 hours | 12 leads (10 electrodes) | Store and forward | Full spatial ECG; ischemia assessment | High electrode burden; more data volume | Mortara H12+ |
| Patch Monitor | 7–14 days | 1–2 channels | Store and forward (mail-in) | Long wear; wire-free; high compliance | No real-time alerting; limited lead count | iRhythm Zio Patch |
| MCOT | Up to 30 days | 2–3 channels | Real-time cellular transmission | Real-time alerting; immediate clinical response | Higher cost; requires network coverage | CardioNet MCOT |
| Implantable Loop Recorder (ILR) | Up to 3 years | 1 channel (subcutaneous) | Remote wireless (bedside communicator) | Longest monitoring; highest diagnostic yield for syncope | Invasive implant procedure; cost; single lead | Medtronic Reveal LINQ |
The selection of an appropriate monitoring modality is driven by symptom frequency, clinical urgency, patient lifestyle factors, and healthcare system resource constraints. For biomedical engineers, each device type represents a distinct set of engineering trade-offs in form factor, power management, signal quality, data throughput, and wireless communication — making this a rich and rapidly evolving domain within cardiovascular medical device engineering.
6. What are the Main Benefits of the Holter Monitor?
The Holter monitor offers a compelling array of clinical and engineering advantages that have cemented its role as a cornerstone diagnostic tool in cardiology. For biomedical engineers working in cardiac device deployment, maintenance, or design, understanding these benefits is essential to appreciating why the technology continues to be refined and widely adopted across healthcare settings globally.
Non-Invasive Continuous Cardiac Monitoring
Perhaps the most significant benefit of the Holter monitor is that it provides prolonged, continuous cardiac monitoring entirely without invasive procedures. Unlike catheter-based electrophysiology studies or subcutaneous implants, the Holter monitor attaches externally via skin electrodes and poses no surgical risk to the patient. This non-invasive nature dramatically lowers the barrier to use, enabling widespread deployment across outpatient clinics, general practices, and even home settings. For biomedical engineers, this translates to lower device complexity in terms of sterility requirements and implant mechanics, while still delivering diagnostically rich data. The device captures electrical activity continuously over 24 to 48 hours or longer, providing a comprehensive cardiac profile that far exceeds what a standard 12-lead ECG — which typically records only 10 seconds of activity — can offer. For further context on how cardiovascular monitoring devices fit into the broader ecosystem of cardiac care, the article What Are Cardiovascular Devices: All You Need to Know as a Biomedical Engineer provides an excellent reference.
Capturing Intermittent and Transient Arrhythmias
One of the most clinically valuable aspects of Holter monitoring is its ability to detect intermittent arrhythmias that would otherwise be completely invisible on a brief resting ECG. Conditions such as paroxysmal atrial fibrillation, Wolff-Parkinson-White syndrome, and transient complete heart block may manifest only sporadically — sometimes for just a few seconds per day — making them nearly impossible to capture without extended recording. The Holter monitor bridges this diagnostic gap by recording all cardiac events over the monitoring period, allowing clinicians to correlate specific ECG findings with the patient’s symptom diary entries. This symptom-rhythm correlation is diagnostically powerful: it allows physicians to confirm or exclude an arrhythmic cause for symptoms such as palpitations, syncope, dizziness, and unexplained dyspnea.
Ambulatory Design and Cost-Effectiveness
The ambulatory design of the Holter monitor allows patients to continue their normal daily activities — including work, exercise, and sleep — while the device records. This is a critical advantage because many arrhythmias are triggered by physical exertion, emotional stress, or postural changes that would not be replicated in a clinical environment. The ability to monitor patients in their natural environment increases diagnostic yield considerably. From an economic standpoint, Holter monitors are significantly more cost-effective than inpatient telemetry monitoring or electrophysiology laboratory studies. The relatively low unit cost, reusable recorder designs, and rapid turnaround in analysis make it an accessible tool for healthcare systems at all resource levels. Biomedical engineers involved in hospital procurement and technology assessment should factor in these cost-effectiveness metrics alongside clinical utility when evaluating ambulatory monitoring solutions.
- Detects arrhythmias missed by standard 10-second 12-lead ECG recordings
- Enables direct symptom-to-ECG correlation via patient activity diary
- Non-invasive with no surgical risk or sterility requirements
- Ambulatory design captures activity-triggered and positional arrhythmias
- Cost-effective compared to inpatient telemetry or electrophysiology studies
- Compatible with outpatient, clinic, and home-based deployment models
7. What are the Risks and Limitations of the Holter Monitor?
While the Holter monitor is a powerful diagnostic instrument, biomedical engineers and clinical staff must remain fully aware of its inherent limitations and potential sources of error. Understanding these constraints is critical for proper device selection, setup optimization, patient preparation, and data interpretation. Several factors can compromise signal quality, reduce diagnostic yield, or introduce safety considerations that must be systematically managed.
Limited Recording Duration and Missed Infrequent Events
The traditional 24- to 48-hour Holter recording window, while significantly longer than a standard ECG, remains insufficient for detecting truly infrequent arrhythmic events. Patients who experience symptoms only once or twice per week — or even less frequently — are unlikely to have their arrhythmia captured within such a short monitoring window. This limitation directly affects diagnostic sensitivity for conditions such as rare paroxysmal atrial fibrillation episodes or infrequent pre-syncope events. The consequence of a missed arrhythmia can be clinically significant, potentially delaying appropriate treatment. Biomedical engineers must understand this limitation when advising on device selection, recognizing that extended-wear devices or implantable loop recorders may be more appropriate for patients with infrequent symptoms. The design principle of matching monitoring duration to arrhythmia frequency is fundamental to effective ambulatory cardiac monitoring strategy.
Signal Artifacts: Motion, EMG, and Electrode Issues
Signal quality is one of the most persistent technical challenges in Holter monitoring. Motion artifacts arise when lead wires or electrodes move relative to the skin during physical activity, introducing noise that can mimic or obscure genuine cardiac events. Electromyographic (EMG) artifacts from skeletal muscle activation — particularly in highly active patients or those with tremors — can contaminate the ECG signal, leading to both false-positive and false-negative arrhythmia detections. Electrode-related problems include skin irritation from adhesive gel, allergic reactions to electrode materials, and gradual degradation of electrode contact over the recording period. Poor skin preparation prior to electrode placement — such as inadequate removal of oils, hair, or dead skin cells — is a leading cause of high impedance and resultant signal noise. Biomedical engineers involved in device training and setup protocols must emphasize proper skin preparation techniques and electrode placement optimization to minimize these artifacts. Just as signal integrity is paramount in other diagnostic imaging modalities — as explored in detail in A comprehensive guide to PACS for biomedical engineers — maintaining clean, artifact-free data is fundamental to reliable Holter analysis.
Patient Compliance, No Real-Time Alerts, and Data Security
Patient compliance represents a significant practical limitation. Patients are required to maintain an accurate activity and symptom diary throughout the monitoring period, yet many fail to record events consistently or accurately, reducing the clinical value of symptom-rhythm correlation. Some patients also remove electrodes prematurely due to discomfort, sweat, or lifestyle factors, truncating the recording. Traditional Holter monitors do not provide real-time alerts to clinicians or patients, meaning that a life-threatening arrhythmia detected on the recording is only identified retroactively after the device is returned and analyzed — a critical safety gap compared to real-time telemetry systems. Furthermore, as Holter systems increasingly transmit data wirelessly or via cloud platforms, data security and HIPAA compliance become important engineering considerations. Biomedical engineers must ensure that data transmission pipelines, storage solutions, and access controls meet applicable regulatory requirements to protect patient privacy and prevent unauthorized access to sensitive cardiac data.
- Traditional 24–48h window may miss infrequent arrhythmic events
- Motion and EMG artifacts can degrade signal quality, especially in active patients
- Electrode skin irritation and adhesive failure reduce long-term signal integrity
- Patient non-compliance with diary keeping reduces diagnostic correlation
- No real-time alerts in traditional models — retrospective analysis only
- Cloud-based platforms introduce HIPAA and cybersecurity compliance requirements
8. How is the Holter Monitor Evolving? Recent Innovations
The Holter monitor has undergone remarkable technological transformation over the past decade, driven by advances in miniaturization, wireless communication, artificial intelligence, and wearable technology. These innovations are fundamentally reshaping ambulatory cardiac monitoring — extending recording durations, improving diagnostic accuracy, enabling real-time data transmission, and integrating seamlessly with consumer electronics. Biomedical engineers at the forefront of cardiac device development must understand these evolving technologies and their implications for device design, regulatory pathways, and clinical deployment.
AI-Powered Arrhythmia Detection and Deep Learning Algorithms
Artificial intelligence has emerged as one of the most transformative forces in Holter monitor evolution. Traditional Holter analysis relied on automated detection algorithms followed by mandatory physician over-reading — a time-intensive process prone to analyst fatigue and inter-reader variability. Contemporary AI-powered platforms, most notably the iRhythm Zio system, employ deep learning algorithms trained on millions of annotated cardiac recordings to detect arrhythmias with sensitivity and specificity approaching or exceeding that of expert cardiologists. Since 2019, the FDA has cleared multiple deep learning algorithms specifically for atrial fibrillation detection from ambulatory ECG data, marking a significant regulatory milestone. These AI systems also incorporate sophisticated noise artifact rejection algorithms that can distinguish genuine arrhythmic events from motion artifact in real time, substantially improving the signal-to-noise ratio of the analyzed data. For biomedical engineers interested in how AI is reshaping medical diagnostics more broadly, the resource Latest Advances of Artificial Intelligence in Healthcare in 2025 offers valuable perspective on this rapidly evolving landscape.
Extended-Wear Patch Monitors and Implantable Loop Recorders
Extended-wear patch monitors represent a paradigm shift in Holter technology. The iRhythm Zio Patch — a single-lead adhesive patch worn continuously for up to 14 days — eliminates the lead wires and external recorder that characterize traditional Holter devices, dramatically improving patient comfort and compliance. The patch stores data locally and is mailed to a central analysis center upon removal, where AI-assisted analysis generates a comprehensive arrhythmia report. For patients requiring even longer monitoring, 30-day event monitors provide another tier of extended surveillance. At the extreme end of the monitoring duration spectrum, the Medtronic Reveal LINQ — a subcutaneous implantable loop recorder approximately the size of a paper clip — can monitor cardiac rhythm continuously for up to three years. While technically beyond the traditional definition of a Holter monitor, the LINQ represents the logical extension of ambulatory cardiac monitoring philosophy, targeting patients with very infrequent but clinically significant arrhythmic events. Biomedical engineers evaluating these devices must consider the engineering tradeoffs between battery life, data storage capacity, transmission bandwidth, and device form factor.
Wireless Transmission, Smartphone Integration, and Wearable ECG
Modern Holter systems increasingly incorporate Bluetooth-enabled transmitters that stream ECG data wirelessly to paired smartphones or cloud-based monitoring platforms, enabling near-real-time physician review and alert generation — directly addressing one of the most critical limitations of traditional Holter technology. Smartphone-integrated Holter analysis apps allow patients and clinicians to review waveforms, annotate events, and receive automated arrhythmia notifications from any location. Consumer wearable devices have also entered the cardiac monitoring space in a clinically meaningful way: the Apple Watch Series 4 and later, along with Samsung Galaxy Watch ECG-enabled models, provide single-lead ECG recordings that have received FDA clearance for atrial fibrillation screening. While these consumer devices do not replace diagnostic-grade Holter monitors, they extend the reach of cardiac surveillance to populations who would not otherwise undergo formal monitoring. Cloud-based remote cardiac monitoring platforms aggregate data from multiple patients simultaneously, enabling scalable population-level arrhythmia surveillance. The ethical dimensions of such pervasive monitoring — including data ownership, algorithmic bias, and equitable access — are important considerations for biomedical engineers, as explored in Ethical Considerations in Biomedical Engineering: Balancing Innovation and Patient Safety. Engineers developing or deploying these platforms must also ensure compliance with EDF+ data format standards, HIPAA data security requirements, and applicable FDA regulations.
- AI deep learning algorithms (e.g., iRhythm Zio) achieve cardiologist-level arrhythmia detection accuracy
- FDA-cleared AI algorithms for AFib detection available since 2019
- 14-day Zio Patch and 30-day event monitors extend recording duration significantly
- Medtronic Reveal LINQ implantable loop recorder enables up to 3-year monitoring
- Bluetooth-enabled real-time data transmission addresses traditional monitoring gaps
- Apple Watch and Samsung Galaxy Watch provide FDA-cleared consumer AFib screening
- Cloud platforms enable scalable population-level remote cardiac monitoring
9. Key Takeaways and Tips for Biomedical Engineers
For biomedical engineers working with Holter monitors — whether in clinical engineering, device design, regulatory affairs, or research — a thorough technical grounding in the device’s engineering principles, operational requirements, and regulatory framework is indispensable. The following section synthesizes the most important practical insights derived from the preceding analysis, providing actionable guidance for engineers across the full device lifecycle.
Signal Quality, Electrode Placement, and Sampling Rate Considerations
Signal quality is the single most important determinant of Holter monitor diagnostic value, and it begins with proper electrode placement and skin preparation. Engineers responsible for device setup training should ensure that clinical staff understand the importance of thorough skin abrasion, defatting with alcohol, and correct anatomical positioning of electrodes to minimize impedance and maximize signal amplitude. The Nyquist sampling theorem is a critical engineering principle that directly governs Holter recorder design: to faithfully reconstruct the highest frequency components of the ECG signal — including the high-frequency components of the QRS complex, which can reach up to 150 Hz — the sampling rate must be at least twice the maximum signal frequency. In practice, diagnostic-grade Holter recorders typically sample at 200 to 1000 Hz, with higher rates preferred for applications requiring precise ST-segment analysis or QRS morphology characterization. Engineers evaluating or specifying Holter systems must verify that the device’s sampling rate meets AAMI EC38 and IEC 60601-2-47 requirements for the intended clinical application. Understanding how device classification and technical standards interact is also essential — a subject addressed comprehensively in How Biomedical Devices Are Classified: Insights into FDA Classification.
Data Formats, Storage, and Regulatory Compliance
Data interoperability is an increasingly important engineering consideration as Holter systems are integrated into electronic health records (EHRs) and multivendor analysis platforms. The European Data Format Plus (EDF+) is the recommended open standard for storing and transmitting biological and physiological signal data, including ambulatory ECG recordings. Engineers specifying Holter systems for hospital deployment should verify EDF+ compatibility to ensure seamless data exchange between recording hardware, analysis software, and clinical information systems. From a regulatory standpoint, Holter monitors in the United States are subject to FDA 21 CFR 870.2340 for ambulatory ECG electrodes and broader Class II device requirements, requiring 510(k) premarket notification. Quality management system compliance with ISO 13485 is mandatory for manufacturers, and engineers working in device development roles should be thoroughly familiar with both the technical documentation requirements and post-market surveillance obligations this standard entails. For cloud-based Holter platforms transmitting patient data over networks, HIPAA Security Rule compliance — including encryption of data in transit and at rest, access controls, and audit logging — is non-negotiable. Biomedical engineers should work closely with IT security teams and compliance officers to architect data pipelines that meet these requirements. Those interested in how regulatory bodies and standards organizations shape the medical device landscape will find valuable context in Key Organizations and Bodies in the Medical Device Field.
Clinical Engineering Best Practices and Career Development
Biomedical engineers supporting Holter monitor programs in clinical environments should establish robust preventive maintenance protocols, including periodic verification of recorder functionality, electrode shelf-life management, and calibration checks of analysis workstations. When evaluating new Holter technologies for procurement, engineers should conduct structured clinical performance assessments that compare sensitivity and specificity for key arrhythmia classes, assess artifact rejection capabilities, and evaluate workflow integration with existing clinical systems. The rapid integration of AI into Holter analysis also demands that biomedical engineers develop literacy in machine learning validation methodologies — understanding concepts such as training data bias, algorithm generalizability across patient populations, and the importance of prospective clinical validation studies. Engineers who can bridge the gap between algorithm development and clinical deployment will be exceptionally valuable as healthcare systems adopt AI-powered cardiac monitoring at scale. For those looking to build the multidisciplinary competencies required for this role, the resource Top Skills Every Biomedical Engineer Should Master provides a helpful development framework. Similarly, the connection between the Holter monitor and the broader family of electrocardiographic devices is well illustrated by exploring the foundational Electrocardiograph (ECG) device overview, which contextualizes how ambulatory monitoring extends the capabilities of standard ECG technology.
- Ensure sampling rates meet Nyquist requirements: minimum 200 Hz, preferably 500–1000 Hz for morphological analysis
- Prioritize skin preparation (abrasion, defatting) to minimize electrode impedance and motion artifact
- Verify EDF+ data format compatibility for interoperability with EHR and analysis platforms
- Confirm FDA 21 CFR 870.2340, AAMI EC38, and IEC 60601-2-47 compliance for all deployed systems
- Implement HIPAA-compliant encryption and access controls for all cloud-based data transmission
- Establish preventive maintenance schedules covering recorder calibration, electrode inventory, and software updates
- Develop AI algorithm validation literacy to critically assess manufacturer performance claims
- Match monitoring duration to arrhythmia frequency — consider extended-wear or implantable options for infrequent events
References
- Zimetbaum, P. J., & Josephson, M. E. (1999). The evolving role of ambulatory arrhythmia monitoring in general clinical practice. Annals of Internal Medicine, 130(10), 848–856. https://doi.org/10.7326/0003-4819-130-10-199905180-00015
- Turakhia, M. P., et al. (2013). Diagnostic utility of a novel leadless arrhythmia monitoring device. The American Journal of Cardiology, 112(4), 520–524. https://doi.org/10.1016/j.amjcard.2013.04.021
- Hannun, A. Y., et al. (2019). Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nature Medicine, 25(1), 65–69. https://doi.org/10.1038/s41591-018-0268-3
- Association for the Advancement of Medical Instrumentation. (2014). AAMI EC38: Ambulatory Electrocardiographs. AAMI. https://www.aami.org/
- International Electrotechnical Commission. (2012). IEC 60601-2-47: Particular requirements for the basic safety and essential performance of ambulatory electrocardiographic systems. IEC. https://www.iec.ch/
- U.S. Food and Drug Administration. (2022). 21 CFR Part 870.2340 — Ambulatory electrocardiograph (Holter monitor) electrode. FDA. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?FR=870.2340
- Isakadze, N., & Martin, S. S. (2020). How useful is the smartwatch ECG? Trends in Cardiovascular Medicine, 30(7), 442–448. https://doi.org/10.1016/j.tcm.2019.10.010
- Medtronic. (2023). Reveal LINQ Insertable Cardiac Monitor — Product overview and technical specifications. Medtronic Inc. https://www.medtronic.com/
- iRhythm Technologies. (2023). Zio AT and Zio Monitor: Clinical evidence and technical overview. iRhythm Technologies, Inc. https://www.irhythmtech.com/
- International Organization for Standardization. (2016). ISO 13485: Medical devices — Quality management systems — Requirements for regulatory purposes. ISO. https://www.iso.org/standard/59752.html
