
The mammography systems Explained for Biomedical Engineers
The mammography system stands as one of the most critical diagnostic tools in modern medical imaging, enabling early detection of breast abnormalities with remarkable precision. As a specialized low-dose X-ray modality, it occupies a unique niche within the broader landscape of radiological devices that biomedical engineers must understand thoroughly. From the physics of differential X-ray attenuation to the engineering of high-resolution flat-panel detectors, mammography systems integrate sophisticated hardware, software, and regulatory frameworks. This article provides a comprehensive technical overview tailored specifically for biomedical engineers working in clinical environments, device development, or regulatory affairs.

- What is the Mammography System?
- Why is the Mammography System used?
- How does the Mammography System work in general?
- What are the main components of the Mammography System?
- What types/variants of Mammography Systems exist?
- What are the main benefits of the Mammography System?
- What are the general risks or limitations of the Mammography System?
- How is the Mammography System evolving / recent innovations?
- Key takeaways / tips for biomedical engineers
1. What is the Mammography System?
Definition and Core Concept
A mammography system is a dedicated medical X-ray imaging device engineered specifically to produce high-resolution, low-dose radiographic images of breast tissue. Unlike conventional general-purpose X-ray machines, mammography systems are optimized for the unique physical and compositional characteristics of the breast, which is composed primarily of glandular tissue, adipose (fatty) tissue, and connective stroma. These tissues exhibit relatively subtle differences in X-ray attenuation, requiring highly sensitive detection systems and carefully calibrated low-energy photon beams to generate diagnostic contrast. The system operates in a voltage range of approximately 22 to 35 kilovolts peak (kVp), substantially lower than the 60–120 kVp used in standard radiography, allowing differentiation between soft tissue structures that would otherwise appear indistinguishable at higher energies.
Historical Development
Mammography has evolved significantly since its inception in the early 1960s, when Dr. Robert Egan introduced standardized screen-film techniques. The modality transitioned through several technological generations: from analog screen-film systems to computed radiography (CR), then to full-field digital mammography (FFDM) in the early 2000s, and most recently to digital breast tomosynthesis (DBT) and contrast-enhanced mammography (CEM). Each generation brought improvements in image quality, radiation dose management, and diagnostic accuracy. Today’s systems incorporate sophisticated digital detectors, automated exposure control, and AI-assisted image analysis, making mammography one of the most technologically advanced modalities in routine clinical use.
Role Within the Medical Imaging Ecosystem
Within the broader imaging ecosystem, mammography occupies a complementary role alongside modalities such as ultrasound, MRI, and, in specialized contexts, PET scanning. It remains the gold-standard first-line screening tool for breast cancer detection in women over 40, endorsed by major health organizations worldwide. For biomedical engineers, understanding its positioning within a multi-modality diagnostic pathway is essential for system integration, workflow optimization, and ensuring interoperability with picture archiving and communication systems (PACS).
2. Why is the Mammography System used?
Early Detection of Breast Cancer
The primary clinical justification for mammography is its proven ability to detect breast cancer at early, more treatable stages — often before a palpable lump develops. Population-level screening programs have demonstrated that regular mammographic screening can reduce breast cancer mortality by approximately 20–40% in screened populations. The modality is uniquely sensitive to microcalcifications, which are tiny calcium deposits that can be the earliest radiographic indicator of ductal carcinoma in situ (DCIS) or invasive carcinoma. These calcification clusters, often measuring only 0.1–1 mm in diameter, are virtually impossible to detect by physical examination or ultrasound, underscoring mammography’s irreplaceable diagnostic value.
Diagnostic and Interventional Applications
Beyond population screening, mammography systems are deployed diagnostically to evaluate symptomatic patients presenting with breast lumps, nipple discharge, skin changes, or axillary lymphadenopathy. Diagnostic mammography typically involves additional projections — such as spot compression views and magnification views — to characterize lesions more precisely. Advanced variants like contrast-enhanced mammography (CEM) and DBT further extend diagnostic capabilities, particularly in women with dense breast tissue where standard 2D imaging is limited. Mammography is also integral to image-guided interventional procedures including stereotactic core biopsy, where the system provides real-time coordinate targeting for tissue sampling, directly linking imaging to pathological diagnosis. This connection between imaging and cancer management illustrates how biomedical engineering is advancing cancer diagnosis and treatment.
Regulatory and Public Health Context
Mammography is among the most tightly regulated medical imaging modalities globally. In the United States, the Mammography Quality Standards Act (MQSA) under FDA 21 CFR Part 900 mandates accreditation, equipment performance standards, personnel qualifications, and quality assurance protocols for every mammography facility. This regulatory framework underscores the public health significance of the modality and creates a structured environment within which biomedical engineers must operate. Understanding how biomedical devices are classified by the FDA is therefore essential for engineers involved in mammography system procurement, installation, or maintenance, as non-compliance carries significant legal and clinical consequences.
3. How does the Mammography System work in general?
Differential X-Ray Attenuation and Beam Physics
The fundamental operating principle of mammography is differential X-ray attenuation across breast tissue types. When a low-energy X-ray beam — typically generated at 25–32 kVp — passes through compressed breast tissue, different tissue components attenuate photons to varying degrees. Glandular and fibrous tissues are denser and attenuate more photons (appearing whiter on the image), whereas adipose tissue is less attenuating (appearing darker). Malignant masses often exhibit increased density relative to surrounding tissue, and microcalcifications produce characteristic high-attenuation spots. The use of low-energy beams is critical: the photoelectric effect dominates at these energies, maximizing subject contrast between adjacent soft tissues that would otherwise produce minimal differential attenuation at higher kVp values used in conventional radiography.
Breast Compression and Scatter Reduction
Breast compression is a non-negotiable element of the mammographic technique. A motorized compression paddle applies controlled force — typically up to 100 Newtons (approximately 10 kg-force) — to flatten the breast against the detector surface. This serves multiple critical engineering and clinical purposes. First, it reduces breast thickness, decreasing the path length that X-rays must traverse, which directly lowers patient radiation dose. Second, compression separates overlapping tissue structures, reducing superimposition artifacts that could mask or mimic lesions. Third, it reduces the production of scattered radiation, which degrades image contrast and introduces noise. Anti-scatter grids — linear or focused grids with high grid ratios (typically 3.5:1 to 5:1) — are positioned between the breast and detector to further absorb obliquely scattered photons, ensuring that only primary beam photons contribute to image formation.
Automatic Exposure Control (AEC) and Parameter Optimization
Modern mammography systems employ sophisticated Automatic Exposure Control (AEC) systems to optimize imaging parameters for each individual patient. The process begins with a brief pre-exposure sampling phase lasting approximately 100 milliseconds, during which the system measures the attenuation characteristics of the compressed breast. Based on this pre-exposure data, the AEC algorithm selects the optimal combination of tube voltage (kVp), tube current–time product (mAs), anode material (molybdenum or rhodium), and beam filtration to achieve the target mean glandular dose (MGD) while maintaining diagnostic image quality. This automated optimization is particularly important given the wide variability in breast thickness (25–100 mm) and tissue composition among patients. The system continuously balances the competing demands of image contrast, spatial resolution, noise, and radiation dose, representing one of the more complex real-time optimization challenges in diagnostic imaging engineering. This principle of optimized exposure shares conceptual roots with AEC systems used in CT scanners, though mammography’s requirements for ultra-low dose and high soft-tissue contrast demand far more precise calibration.
4. What are the main components of the Mammography System?
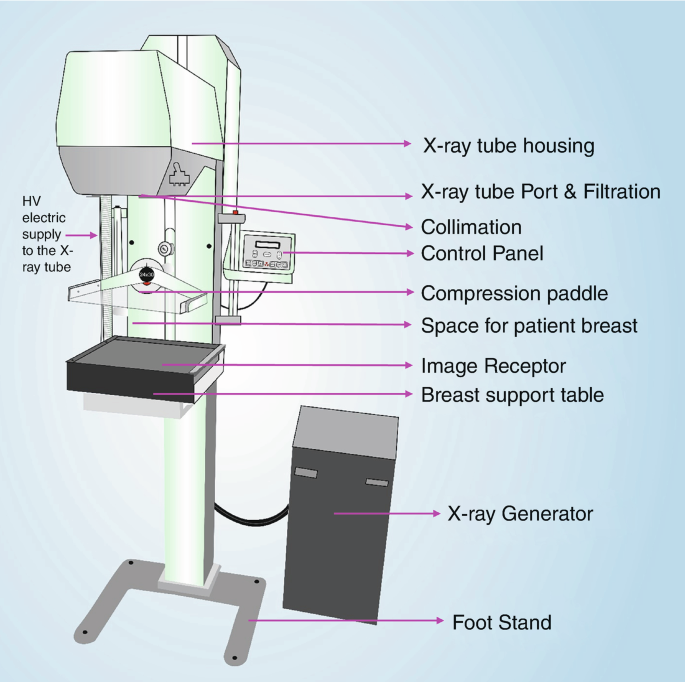
X-Ray Tube and Anode-Filter Combinations
The X-ray tube in a mammography system is a specialized component fundamentally distinct from those used in general radiography. It features dedicated anode target materials — primarily molybdenum (Mo) and rhodium (Rh) — chosen for their characteristic X-ray emission spectra in the 17–23 keV range, which are ideally suited to breast tissue imaging. Molybdenum anodes produce characteristic radiation at 17.5 and 19.6 keV, optimizing contrast for average-density breasts. Rhodium anodes emit slightly higher-energy characteristic photons (~20.2 and 22.7 keV), better suited for thicker or denser breasts. Some modern systems also incorporate tungsten (W) anodes with appropriate filtration for digital detectors. The focal spot size is critically small — typically 0.3 mm for standard views and 0.1 mm for magnification views — to achieve the high spatial resolution (≥10 line pairs per mm) needed to resolve microcalcifications. The tube assembly mounts on a rotating C-arm gantry that can swing through a full arc, enabling multiple projection angles without patient repositioning.
Compression Paddle and Positioning Mechanics
The compression paddle is a rigid, radiolucent plate — typically constructed from polycarbonate — driven by a motorized mechanism capable of applying compression forces up to 100 N under automatic mode, with manual override capability. Modern paddles incorporate load-cell sensors providing real-time force feedback to the operator display, ensuring reproducible and safe compression levels. The paddle geometry varies: standard flat paddles for routine views, spot compression paddles for focused lesion evaluation, and fenestrated paddles for biopsy access. Proper compression is a major determinant of image quality and dose; an inadequately compressed breast results in increased scatter, motion blur from physiological movement, and higher radiation dose. Biomedical engineers performing quality assurance must regularly calibrate compression force accuracy (typically ±20 N tolerance) and verify paddle flex compliance to maintain system performance.
Flat-Panel Digital Detector
The image receptor in modern mammography systems is an amorphous silicon (a-Si) or amorphous selenium (a-Se) flat-panel detector. Direct-capture detectors (a-Se) convert X-ray photons directly into electrical charge without an intermediate light conversion step, offering superior spatial resolution (pixel pitch as small as 50–70 µm). Indirect-capture detectors use a cesium iodide (CsI) scintillator phosphor layer to convert X-rays into visible light, which is then captured by a CCD or photodiode array. The large active area (typically 24×30 cm or 24×29 cm) must cover the full breast field without stitching artifacts. Key detector performance metrics for biomedical engineers include detective quantum efficiency (DQE), modulation transfer function (MTF), noise power spectrum (NPS), and the signal-difference-to-noise ratio (SDNR) — all of which must meet ACR and FDA performance thresholds under routine quality control testing.
AEC System and Generator
The AEC system integrates ion chambers or detector-based sensors positioned beneath the breast to sample transmitted beam intensity during the pre-exposure phase. The high-frequency generator — capable of delivering precisely controlled short exposures (typically 0.5–3 seconds) at milliampere currents of 25–200 mA — responds rapidly to AEC commands to terminate exposure at the optimal mAs endpoint. Modern generators operate at high switching frequencies (>5 kHz), ensuring minimal kVp ripple (<2%) and reproducible dose delivery. The entire exposure control chain — from pre-sampling through parameter selection to exposure termination — must be validated and documented as part of annual physics testing required by MQSA regulations. Integration of generator performance data into the facility’s quality management system is a core responsibility for clinical biomedical engineers maintaining mammography equipment.
5. What types/variants of Mammography Systems exist?
2D Screen-Film Mammography (SFM)
Screen-film mammography (SFM) represents the analog foundation of the modality, using a rare-earth intensifying screen coupled with single-emulsion film as the image receptor. While largely supplanted by digital systems in high-income countries, SFM remains operational in resource-limited settings. It offers high spatial resolution inherent to film grain structure, but is constrained by a narrow exposure latitude, requiring precise exposure control to avoid under- or over-exposure. Film processing chemistry introduces variability and requires strict quality control. The critical limitation is the two-dimensional projection nature of the image: superimposition of overlapping tissue structures generates both false positives (summation artifacts mimicking masses) and false negatives (real lesions obscured by overlying tissue), particularly problematic in women with heterogeneously dense breasts.
Full-Field Digital Mammography (FFDM)
FFDM replaced screen-film as the clinical standard by the mid-2000s, employing large-area flat-panel detectors to capture digital images with superior dynamic range and post-processing flexibility. Digital images can be manipulated — windowing, leveling, magnification — without repeat exposure, reducing recall rates. Large clinical trials (notably the DMIST trial) demonstrated FFDM’s superiority over SFM in pre-menopausal women and women with dense breasts. FFDM integrates seamlessly with PACS infrastructure and CAD (computer-aided detection) software. Leading FFDM platforms include GE Healthcare’s Senographe Pristina and Siemens Healthineers’ MAMMOMAT Revelation, both of which incorporate ergonomic design innovations to improve patient comfort and positioning accuracy, which directly influences image quality and diagnostic yield.
Digital Breast Tomosynthesis (DBT / 3D Mammography)
DBT represents the most significant engineering advancement in mammography since digitization. The X-ray tube sweeps through a limited arc of 15–60° (varying by manufacturer), acquiring 9–50 low-dose projection images at discrete angles. These projections are mathematically reconstructed — using filtered back-projection or iterative reconstruction algorithms similar in concept to those employed in CT scanners — into a series of thin (1 mm) tomographic slabs through the breast volume. This pseudo-3D representation effectively eliminates the tissue superimposition problem that plagues conventional 2D mammography, substantially improving cancer detection rates (sensitivity increased by 15–40% in some studies) and reducing false-positive recall rates. Hologic’s Selenia Dimensions and 3Dimensions systems pioneered commercial DBT, while GE’s SenoClaire and Siemens’ MAMMOMAT Inspiration have introduced proprietary reconstruction approaches with varying angular sweep geometries and tube motion strategies.
Contrast-Enhanced Mammography (CEM)
CEM combines standard mammographic technique with intravenous iodinated contrast agent injection to exploit the differential vascular enhancement of malignant lesions. The technique acquires paired low-energy (26–31 kVp) and high-energy (45–49 kVp) images; dual-energy subtraction processing removes the background parenchymal signal, leaving a subtracted image that highlights iodine-enhancing lesions. CEM demonstrates comparable diagnostic performance to breast MRI for lesion characterization in dense breasts, at significantly lower cost and with shorter examination time. It is particularly valuable in evaluating biopsy-proven cancers (extent of disease), assessing treatment response, and characterizing indeterminate lesions on standard mammography. The modality requires a contrast injection protocol, patient screening for renal function and contrast allergy, and integration with a dual-energy capable X-ray generator — all considerations that fall within the biomedical engineer’s scope during system procurement and commissioning.
Comparison Table of Mammography System Types
| Type | Detector Technology | Image Dimensionality | Key Advantage | Key Limitation | Typical kVp Range | Representative Manufacturers |
|---|---|---|---|---|---|---|
| Screen-Film (SFM) | Rare-earth screen + film | 2D projection | High intrinsic spatial resolution; low cost | Narrow latitude; tissue superimposition; no post-processing | 25–32 kVp | Legacy Kodak, Agfa |
| Full-Field Digital (FFDM) | a-Se or CsI/a-Si flat panel | 2D projection | Wide dynamic range; post-processing; PACS integration | Tissue superimposition remains; reduced contrast in dense breasts | 25–35 kVp | GE Senographe Pristina, Siemens MAMMOMAT, Fujifilm AMULET |
| Digital Breast Tomosynthesis (DBT) | a-Se or CsI flat panel (motion-tolerant) | Pseudo-3D (1 mm slabs) | Eliminates tissue superimposition; higher sensitivity/specificity | Increased dose vs. 2D alone; longer read time; higher cost | 25–35 kVp (multi-angle) | Hologic Selenia/3Dimensions, GE SenoClaire, Siemens MAMMOMAT Inspiration |
| Contrast-Enhanced (CEM) | Dual-energy capable flat panel | 2D subtracted (functional) | Lesion vascularity characterization; near-MRI diagnostic performance | IV contrast risks; higher dose than standard 2D; renal screening required | 26–31 kVp (low) / 45–49 kVp (high) | GE Senographe Pristina, Hologic 3Dimensions, Siemens MAMMOMAT |
6. What Are the Main Benefits of the Mammography System?
6.1 Early Cancer Detection and Mortality Reduction
The most clinically significant benefit of mammography is its ability to detect breast cancer at an early, treatable stage — often before a palpable lump develops. Large-scale randomized controlled trials and meta-analyses consistently demonstrate that regular mammographic screening reduces breast cancer mortality by approximately 20–40% in women aged 40–74. Detection of ductal carcinoma in situ (DCIS) and small invasive tumors dramatically improves prognosis and increases the likelihood of breast-conserving surgery over mastectomy. This directly aligns with the broader mission of biomedical engineering in advancing cancer diagnosis and treatment. Early-stage detection also reduces the need for aggressive chemotherapy regimens, lowering overall healthcare burden and improving quality of life for patients.
6.2 High Spatial Resolution and Non-Invasive Acquisition
Modern mammography systems achieve exceptional spatial resolution of 50–100 µm, enabling visualization of microcalcifications — clusters of calcium deposits as small as 0.1 mm that may indicate early malignancy. This resolution is achieved through high-resolution flat-panel detectors with pixel pitches of 70–100 µm and optimized X-ray tube focal spot sizes (0.1–0.3 mm). Crucially, mammography is entirely non-invasive, requiring no contrast injection or sedation for standard screening. Exams are completed within minutes, making it a practical modality for large-scale population screening programs worldwide.
6.3 Cost-Effectiveness, Digital Workflow, and CAD Integration
Mammography remains one of the most cost-effective cancer screening tools available. Compared to MRI or PET-CT, equipment and operational costs are substantially lower, enabling widespread deployment in community clinics, mobile units, and resource-limited settings. Full-field digital mammography (FFDM) systems facilitate rapid image transfer via DICOM-compliant PACS networks, supporting teleradiology and remote reading workflows. Integration with Computer-Aided Detection (CAD) tools enhances radiologist performance, particularly in high-volume screening environments. Digital systems also permit post-processing adjustments — window/level optimization, noise reduction, and magnification — without repeat exposure. Digital Breast Tomosynthesis (DBT) further reduces recall rates by 15–40% compared to 2D mammography, directly decreasing unnecessary patient anxiety and healthcare costs associated with false-positive callbacks.
7. What Are the General Risks or Limitations of the Mammography System?
7.1 Ionizing Radiation Exposure and Cumulative Risk
Mammography involves ionizing radiation, delivering a mean glandular dose (MGD) of approximately 2–4 mGy per standard two-view examination. While this is low in absolute terms, cumulative exposure from annual screening over decades raises theoretical concerns about radiation-induced carcinogenesis, particularly in younger women with longer latency periods. For women undergoing annual screening from age 40 to 74, the cumulative dose approaches 70–140 mGy. Regulatory standards enforced by the FDA under 21 CFR Part 900 (MQSA) mandate strict dose limits and quality assurance protocols to minimize unnecessary exposure. Biomedical engineers play a key role in designing dose optimization algorithms, including automatic exposure control (AEC) systems and photon-counting detector architectures, which significantly reduce patient dose without sacrificing image quality.
7.2 False Positives, False Negatives, and Dense Breast Tissue
Two-dimensional mammography carries a false positive recall rate of approximately 10% per screening round in the United States, meaning a substantial proportion of women are called back for additional imaging or biopsy despite having no malignancy. This leads to significant patient anxiety, unnecessary procedures, and healthcare costs. Conversely, false negatives — missed cancers — occur in approximately 10–20% of cases, most commonly in women with dense breast tissue. Dense fibroglandular tissue appears white on mammograms, as does tumor tissue, creating a masking effect that reduces sensitivity to as low as 30–48% in extremely dense breasts. Women with heterogeneously dense or extremely dense breast tissue (approximately 40–50% of the screening population) may benefit from supplemental imaging modalities such as ultrasound or MRI. These limitations underscore the importance of volumetric breast density assessment tools and informed patient communication in modern screening programs.
7.3 Compression Discomfort, Special Populations, and Specificity Constraints
Breast compression during mammography, typically to 10–15 kg of applied force, is a significant source of patient discomfort and anxiety, contributing to screening non-compliance. Compression is essential to reduce tissue thickness, decrease scatter radiation, improve contrast, and minimize motion blur — yet it remains a persistent barrier to uptake. Special populations present additional challenges: women with breast implants require modified displacement views (Eklund technique) and specialized positioning that increases complexity and examination time. Young women under 40 are generally not recommended for routine mammographic screening due to greater radiation sensitivity, higher breast density, and lower background prevalence of cancer. Mammography also demonstrates limited specificity; a positive finding requires histopathological confirmation via biopsy. Positive predictive values for biopsy recommendation range from approximately 25–40%, meaning the majority of biopsied lesions are ultimately benign. Biomedical engineers and clinicians must carefully weigh these trade-offs when evaluating screening guidelines and system performance metrics, mindful of the ethical considerations in balancing innovation and patient safety.
8. How Is the Mammography System Evolving? Recent Innovations
8.1 Digital Breast Tomosynthesis and Photon-Counting Mammography
Digital Breast Tomosynthesis (DBT) has rapidly emerged as the new clinical standard in breast screening. By acquiring multiple low-dose projection images across an angular arc (typically 15°–50°) and reconstructing pseudo-3D image slices (1 mm thickness), DBT dramatically reduces the tissue superimposition that plagues 2D mammography. Clinical studies demonstrate that DBT combined with 2D mammography (or synthetic 2D reconstructions) increases cancer detection rates by 20–65% while reducing recall rates by 15–40%. Systems such as the Hologic Selenia Dimensions and 3Dimensions, and GE Healthcare Senographe Pristina, lead the commercial market. Photon-counting mammography (PCM) represents a further leap forward. The Siemens MAMMOMAT Revelation employs silicon photon-counting detectors that individually count and energy-discriminate incoming X-ray photons, eliminating electronic noise entirely. PCM delivers superior contrast-to-noise ratio at significantly reduced dose — approximately 40–50% lower MGD compared to conventional flat-panel systems — while simultaneously enabling spectral imaging for improved tissue characterization. For engineers, photon-counting architectures represent a fundamental paradigm shift in detector design, replacing scintillator-photodiode stacks with direct-conversion semiconductor arrays.
8.2 Artificial Intelligence, Deep Learning CAD, and Radiomics
Artificial intelligence is transforming mammographic interpretation at every level. Deep learning-based CAD platforms — including Hologic Genius AI, iCAD ProFound AI, and Volpara Analytics — are trained on millions of annotated mammograms and can detect malignant lesions, classify breast density, and triage worklist priority with sensitivity and specificity approaching or exceeding that of experienced radiologists. These systems leverage convolutional neural networks (CNNs) and vision transformers operating on full-resolution DICOM images, identifying subtle patterns of mass morphology, spiculation, and microcalcification architecture. Radiomics extends AI further, extracting hundreds of quantitative imaging features from regions of interest to predict tumor biology, receptor status, and treatment response — moving mammography from purely anatomical screening toward functional characterization. Biomedical engineers with strong skills in machine learning, signal processing, and medical imaging are at the forefront of developing and validating these algorithms for clinical deployment.
8.3 Contrast-Enhanced Spectral Mammography, Automated Breast Ultrasound, and MBI
Contrast-Enhanced Spectral Mammography (CESM) injects iodinated contrast medium intravenously and acquires dual-energy mammographic images, leveraging the contrast uptake of hypervascular tumors to dramatically improve lesion conspicuity — particularly in dense breasts. CESM demonstrates sensitivity comparable to breast MRI at a fraction of the cost. Automated Breast Ultrasound (ABUS) systems provide whole-breast coronal and axial volumetric ultrasound imaging as a standardized supplement to mammography in dense-breast populations, removing operator dependency inherent in handheld ultrasound. These developments align closely with innovations in advanced ultrasound technologies for medical imaging. Molecular Breast Imaging (MBI) uses gamma cameras with high-resolution CZT detectors to image uptake of Tc-99m sestamibi, providing functional metabolic information about tissue. Volumetric breast density assessment tools (Volpara Density, Hologic Quantra) now provide automated, reproducible ACR density classification from standard mammograms, replacing subjective visual estimation and informing personalized screening recommendations.
9. Key Takeaways and Tips for Biomedical Engineers
9.1 Core Engineering Competencies for Mammography System Development
Biomedical engineers working in mammography must develop expertise spanning multiple technical domains. A thorough understanding of X-ray physics — including spectral shaping with rhodium/molybdenum/tungsten targets and filters, heel effect management, and scatter rejection via anti-scatter grids — forms the essential foundation. Detector physics competency is equally critical: engineers must understand both indirect (CsI scintillator + a-Si photodiode) and direct (a-Se photoconductor) conversion flat-panel detector architectures, their DQE curves, MTF characteristics, and noise power spectra. For photon-counting systems, knowledge of semiconductor detector design (silicon, CdTe, CZT), charge transport modeling, and pulse-processing electronics is increasingly valuable. Proficiency in image processing — filtered back projection and iterative reconstruction for DBT, denoising algorithms, and DICOM compliance — rounds out the core technical skill set necessary for contributions to system design and validation.
9.2 Regulatory Navigation and Quality Assurance
Mammography is one of the most tightly regulated medical imaging modalities in the world. In the United States, all mammography facilities must comply with the Mammography Quality Standards Act (MQSA, 21 CFR Part 900), which mandates annual equipment inspections, physicist surveys, radiologist credentialing, and dose tracking. Mammography X-ray systems are classified as FDA Class II devices (510(k) pathway), and engineers must be familiar with predicate device identification and substantial equivalence arguments — foundational knowledge covered in the context of FDA device classification. Internationally, compliance with IEC 60601-1 (general safety) and IEC 60601-2-45 (mammographic equipment-specific requirements), ACR Mammography Accreditation, and the EUREF European Protocol for Quality Control is essential. ISO 13485 quality management system certification governs the entire design, manufacturing, and post-market surveillance lifecycle. Engineers should build quality by design (QbD) principles into development workflows from the earliest concept stages.
9.3 Emerging Opportunities and Practical Recommendations
The integration of AI into mammography workflows presents significant career opportunities for biomedical engineers with cross-disciplinary expertise in imaging physics, software development, and clinical validation methodology. Key practical recommendations include: (1) prioritize dose optimization in any system design — phantom-based evaluation using ACR or EUREF protocols should be conducted early and iteratively; (2) validate AI algorithms rigorously on diverse, multi-institutional datasets to mitigate demographic bias, particularly across different breast densities and racial/ethnic groups; (3) engage with radiologists and clinicians early in the design process to ensure workflows are intuitive and findings are actionable; (4) maintain awareness of evolving supplemental screening guidelines for dense-breast patients, as legislative mandates (e.g., the US FDA Dense Breast Reporting Rule effective 2023) are reshaping clinical practice and driving demand for density assessment tools; and (5) pursue continuous education in machine learning, regulatory affairs, and human factors engineering — the intersection of these disciplines defines the next generation of mammography innovation. The future of mammography lies in personalized, risk-stratified screening protocols powered by AI, advanced detector technology, and multimodal data integration.
References
- International Electrotechnical Commission. IEC 60601-1: Medical Electrical Equipment — Part 1: General Requirements for Basic Safety and Essential Performance. 3rd ed. Geneva: IEC; 2005 (amended 2012).
- International Electrotechnical Commission. IEC 60601-2-45: Medical Electrical Equipment — Part 2-45: Particular Requirements for the Basic Safety and Essential Performance of Mammographic X-Ray Equipment. 4th ed. Geneva: IEC; 2019.
- U.S. Food and Drug Administration. Mammography Quality Standards Act and Program (MQSA), 21 CFR Part 900. Silver Spring, MD: FDA; 2023. Available at: https://www.fda.gov/radiation-emitting-products/mammography-quality-standards-act-and-program
- American College of Radiology. ACR Mammography Accreditation Program Requirements. Reston, VA: ACR; 2022. Available at: https://www.acr.org/Clinical-Resources/Mammography-Resources
- European Reference Organisation for Quality Assured Breast Screening and Diagnostic Services (EUREF). European Protocol for the Quality Control of the Physical and Technical Aspects of Digital Mammography. 4th ed. Brussels: EUREF; 2013.
- Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499–2507. doi:10.1001/jama.2014.6095
- Siu AL; U.S. Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164(4):279–296. doi:10.7326/M15-2886
- Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353(17):1773–1783. doi:10.1056/NEJMoa052911
- Lång K, Larsson AM, Rokita D, et al. Artificial intelligence-supported screen reading versus standard double reading in the Mammography Screening with Artificial Intelligence trial (MASAI): a clinical safety analysis of a randomised, controlled, non-inferiority, single-blinded, screening accuracy study. Lancet Oncol. 2023;24(8):936–944. doi:10.1016/S1470-2045(23)00298-X
- Bergh J, Jönsson PE, Glimelius B, Nygren P. A systematic overview of chemotherapy effects in breast cancer. Acta Oncol. 2001;40(2–3):253–281.
- National Institute of Biomedical Imaging and Bioengineering (NIBIB). Mammography. Bethesda, MD: NIBIB; 2023. Available at: https://www.nibib.nih.gov/science-education/science-topics/mammography
- Hologic, Inc. Selenia Dimensions and 3Dimensions Mammography Systems. Marlborough, MA: Hologic; 2023. Available at: https://www.hologic.com/hologic-products/breast-skeletal-health-solutions/3dimensions-mammography-system
- GE Healthcare. Senographe Pristina Mammography System. Chicago, IL: GE Healthcare; 2023. Available at: https://www.gehealthcare.com/products/mammography/senographe-pristina
- Siemens Healthineers. MAMMOMAT Revelation Photon-Counting Mammography. Erlangen: Siemens Healthineers; 2023. Available at: https://www.siemens-healthineers.com/mammography/mammomat-revelation
- Fujifilm Medical Systems. AMULET Innovality Digital Mammography System. Stamford, CT: Fujifilm; 2023. Available at: https://www.fujifilm.com/us/en/healthcare/mammography
- ISO. ISO 13485: Medical Devices — Quality Management Systems — Requirements for Regulatory Purposes. Geneva: ISO; 2016.
- Tabar L, Vitak B, Chen TH, et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology. 2011;260(3):658–663. doi:10.1148/radiol.11110469
- Volpara Health. Volpara Density and Analytics Platform. Wellington, NZ: Volpara Health; 2023. Available at: https://www.volparahealth.com
