
What is a Defibrillator – All you need to know as a Biomedical Engineers
A defibrillator is a critical life-saving medical device used to restore a normal cardiac rhythm by delivering a controlled electrical shock to the heart. Found in hospitals, ambulances, public spaces, and even implanted directly inside patients, defibrillators represent one of the most impactful technologies in emergency and cardiac care. For biomedical engineers, understanding the physics, design, regulatory landscape, and evolving innovations of defibrillators is essential for developing, maintaining, and improving these devices. This overview covers the fundamental principles, component architecture, device variants, clinical benefits, known limitations, and the latest technological advancements shaping the future of defibrillation.

- What is a Defibrillator?
- Why is a Defibrillator used?
- How does a Defibrillator work in general?
- What are the main components of a Defibrillator?
- What types/variants of Defibrillator exist?
- What are the main benefits of a Defibrillator?
- What are general risks or limitations?
- How is the Defibrillator evolving / recent innovations?
- Key takeaways / tips for biomedical engineers
1. What is a Defibrillator?
Definition and Core Purpose
A defibrillator is a medical device that delivers a precisely controlled, high-energy electrical shock to the myocardium (heart muscle) with the goal of terminating life-threatening arrhythmias and allowing the heart’s natural pacemaker — the sinoatrial (SA) node — to re-establish a coordinated, normal sinus rhythm. The term “defibrillation” refers specifically to the depolarization of a critical mass of cardiac cells simultaneously, interrupting the chaotic electrical activity known as ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT). These two arrhythmias are the most common immediately treatable causes of sudden cardiac arrest (SCA) and represent the primary indications for defibrillation.
Historical Development
The concept of using electricity to restart a fibrillating heart was demonstrated as early as the 1940s and 1950s, with pioneers such as Paul Zoll and Bernard Lown contributing foundational research. Lown’s development of the DC capacitor-discharge defibrillator in 1962 replaced earlier AC-based devices and became the standard paradigm for decades. The introduction of biphasic waveform technology in the 1990s significantly reduced the energy needed for effective defibrillation, minimizing myocardial damage while improving success rates. Today, defibrillators range from compact automated external defibrillators (AEDs) weighing under 2 kg to sophisticated implantable cardioverter-defibrillators (ICDs) no larger than a matchbox.
Scope in Biomedical Engineering
From a biomedical engineering perspective, the defibrillator sits at the intersection of high-voltage electronics, signal processing, materials science, and clinical physiology. Engineers are involved in capacitor design, waveform optimization, electrode materials research, firmware development for rhythm detection algorithms, and regulatory compliance. The device must also integrate seamlessly with complementary monitoring tools — such as an ECG machine or a cardiac monitor — to accurately assess the cardiac rhythm before, during, and after shock delivery.
2. Why is a Defibrillator used?
Sudden Cardiac Arrest and Ventricular Fibrillation
Sudden cardiac arrest (SCA) kills approximately 350,000–400,000 people annually in the United States alone. The majority of out-of-hospital SCA events are initially caused by ventricular fibrillation or pulseless ventricular tachycardia, both of which are shockable rhythms. In VF, the heart’s electrical signals become completely disorganized, causing the myocardium to quiver rather than contract effectively, resulting in cessation of blood circulation. Without intervention within minutes, irreversible brain damage and death follow. Defibrillation is the definitive treatment for these rhythms; for every minute without defibrillation, survival rates decrease by approximately 7–10%.
Clinical Indications
The primary clinical indications for external defibrillation are ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT). Synchronized cardioversion — a related but distinct procedure — is used for unstable supraventricular tachyarrhythmias such as atrial fibrillation, atrial flutter, and hemodynamically unstable ventricular tachycardia with a pulse. Synchronized shocks are timed to the R-wave of the QRS complex to avoid delivery during the vulnerable T-wave period, which could paradoxically induce VF. Implantable cardioverter-defibrillators (ICDs) are indicated for patients at high risk of recurrent life-threatening arrhythmias, including those with a history of cardiac arrest, severely reduced left ventricular ejection fraction, or inherited arrhythmia syndromes such as Brugada syndrome or long QT syndrome.
Public Access Defibrillation Programs
Public access defibrillation (PAD) programs have placed AEDs in airports, shopping malls, stadiums, schools, and other high-traffic locations to reduce time-to-defibrillation for out-of-hospital cardiac arrest victims. Studies have shown that PAD programs can increase survival rates from out-of-hospital VF by up to 40–50% when AEDs are deployed within 3–5 minutes of collapse and used by trained bystanders. Regulatory bodies in many countries mandate AED placement in certain public facilities, driving strong market growth and continued device miniaturization. Continuous rhythm monitoring using a Holter monitor can also help identify high-risk patients who may benefit from an ICD before a life-threatening event occurs.
3. How does a Defibrillator work in general?

The Physics of Defibrillation
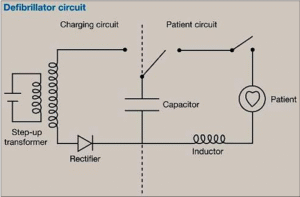
The fundamental operating principle of a defibrillator relies on storing electrical energy in a high-voltage capacitor and then rapidly discharging that energy through the patient’s chest (or directly across the heart in implantable devices). The energy stored in the capacitor is described by the equation E = ½CV², where E is energy in joules (J), C is capacitance in farads (F), and V is voltage in volts. Typical external defibrillators use capacitances ranging from 100 to 500 µF charged to voltages between 1000 V and 3600 V, delivering shock energies of 30–400 J. The delivered energy is determined not only by the stored charge but also by the transthoracic impedance (TTI) of the patient, which typically ranges from 50 to 100 Ω and varies with body composition, electrode size, and electrode contact pressure.
Monophasic vs. Biphasic Waveforms
Early defibrillators used monophasic waveforms, in which current flows in a single direction from one electrode to the other. These devices typically required shock energies of 200–360 J to achieve successful defibrillation. Modern defibrillators use biphasic waveforms, in which current flows in one direction for the first phase (typically 6–10 ms) and then reverses direction for the second phase. The reversal of polarity reduces the defibrillation threshold, allowing effective defibrillation at energies of only 120–200 J — roughly half the energy of monophasic shocks. Lower energy delivery reduces myocardial damage, post-shock dysfunction, and skin burns. Two common biphasic waveform designs are the Biphasic Truncated Exponential (BTE) waveform and the Rectilinear Biphasic (RLB) waveform, each with specific characteristics regarding their response to varying patient impedances.
Rhythm Detection and Shock Decision
Before delivering a shock, defibrillators must analyze the patient’s cardiac rhythm. In manual defibrillators used by trained clinicians, this analysis is performed visually using an integrated ECG display. In AEDs, onboard signal processing algorithms automatically analyze the rhythm acquired through the defibrillation pads, determine whether a shockable rhythm is present, and either advise the operator to press a shock button (semi-automatic AED) or deliver the shock automatically (fully automatic AED). These algorithms analyze features such as QRS morphology, frequency content, amplitude, and regularity to distinguish VF and pVT from non-shockable rhythms like asystole and pulseless electrical activity (PEA). Algorithm sensitivity and specificity are critical performance metrics governed by standards such as IEC 60601-2-4.
4. What are the main components of a Defibrillator?
Energy Storage and Delivery System
The core of any defibrillator is its high-voltage capacitor, which must store large amounts of electrical energy and discharge it in milliseconds. Electrolytic capacitors capable of storing 100–400 J at voltages up to 3600 V are common in external devices. The charging circuit includes a step-up transformer and a high-voltage power supply, which charge the capacitor from a relatively low battery voltage (typically 12–14.8 V) to the required high voltage. The discharge circuit consists of a high-voltage switch (typically an SCR- or IGBT transistor network), inductor coils for waveform shaping, and the discharge pathway through the patient electrodes. In biphasic devices, an H-bridge switching circuit reverses current polarity during the second phase of the waveform.
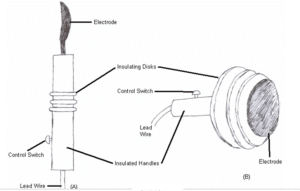
Electrodes and Patient Interface
Defibrillator electrodes (paddles or adhesive pads) serve as the interface between the device and the patient. Traditional reusable paddles are made with stainless steel or titanium contact surfaces and require conductive gel to reduce impedance. Modern single-use adhesive electrode pads incorporate a conductive hydrogel that lowers skin-electrode impedance, improves current distribution, and allows hands-free defibrillation. Electrode placement follows standardized positions: anterolateral (right infraclavicular and left apex) or anteroposterior. For ICDs, titanium-encased electrodes with high-surface-area fractal or platinum-iridium coatings are used to minimize the defibrillation energy threshold while minimizing tissue damage. The impedance measurement circuit continuously monitors electrode contact quality and patient impedance to enable impedance-compensated waveform delivery.
Power Supply, Microelectronics, and Display
External defibrillators are powered by rechargeable lithium-ion (Li) or nickel-cadmium (NiCd) battery packs, designed to deliver a minimum number of shocks (typically 200+ shocks per charge) and support extended monitoring operation. Battery management circuits monitor charge state and provide low-battery warnings critical for emergency readiness. The microcontroller or DSP core manages the charging sequence, rhythm analysis algorithm, waveform generation, user interface, and data logging. An LCD or TFT color display shows the ECG waveform, energy level, device status, and CPR coaching prompts. Many modern devices include wireless communication modules (Wi-Fi, Bluetooth, or cellular) for remote monitoring, incident data transmission, and fleet management. Data storage logs event data including ECG recordings, timestamps, energy delivered, and shock count for post-event analysis and regulatory reporting.
5. What types/variants of Defibrillator exist?
Overview of Defibrillator Categories
Defibrillators are broadly categorized by their intended use environment, level of automation, and whether they are external or implantable. Each category is designed to serve a specific patient population and clinical setting, with engineering trade-offs in size, energy capability, automation, and user interface. The four major categories are: Manual Defibrillators (used in hospitals and by paramedics), Automated External Defibrillators (AEDs, used in public spaces and by first responders), Implantable Cardioverter-Defibrillators (ICDs, surgically implanted for chronic high-risk patients), and Wearable Cardioverter-Defibrillators (WCDs, worn externally for outpatient monitoring). Leading manufacturers include ZOLL Medical, Physio-Control/Stryker, Philips Healthcare, GE Healthcare, Medtronic, and Defibtech.
Comparison Table of Defibrillator Types
| Type | Setting | User | Energy Range | Key Feature |
|---|---|---|---|---|
| Manual Defibrillator | Hospital, ICU, EMS | Trained clinician / paramedic | 30–360 J (biphasic); up to 400 J (monophasic) | Full ECG display, manual energy selection, synchronized cardioversion capability |
| AED (Automated External Defibrillator) | Public spaces, schools, gyms, airports | Layperson / first responder | 120–200 J (biphasic) | Automated rhythm analysis, voice/visual prompts, minimal training required |
| ICD (Implantable Cardioverter-Defibrillator) | Inside patient’s body (chronic) | Autonomous (no user action required) | Up to 40 J (internal) | Continuous 24/7 monitoring, anti-tachycardia pacing, tiered therapy delivery |
| Wearable Cardioverter-Defibrillator (WCD) | Outpatient / post-discharge | Patient (worn on body) | 75–150 J (external) | Non-invasive protection during high-risk period, remote monitoring, activity tracking |
Implantable and Subcutaneous Variants
Traditional transvenous ICDs use leads threaded through the venous system into the heart to sense rhythm and deliver shocks. The subcutaneous ICD (S-ICD), such as the Boston Scientific EMBLEM™, avoids intravascular leads entirely by placing the shock coil subcutaneously along the sternum, eliminating risks of lead-related complications such as perforation, infection, and venous stenosis. Leadless ICDs represent the next frontier, combining pacing and defibrillation in a small capsule anchored directly to the endocardium — though fully leadless defibrillation remains in active clinical development. The Medtronic Micra™ platform has inspired development toward leadless ICD systems that could deliver therapy without any transvenous leads whatsoever. These advances are driven by the desire to reduce long-term lead complications while maintaining reliable rhythm therapy.
6. What are the main benefits of a Defibrillator?
Life-Saving Efficacy in Cardiac Arrest
The most compelling benefit of defibrillators is their proven ability to save lives from sudden cardiac arrest. When VF or pVT is the presenting rhythm and defibrillation is performed within the first few minutes, survival rates can exceed 50–70% in witnessed cardiac arrest scenarios in controlled settings. The combined protocol of early CPR and rapid defibrillation — the cornerstone of the Chain of Survival established by the American Heart Association (AHA) — has been shown to dramatically improve neurologically intact survival outcomes. In hospital settings, rapid defibrillation by trained staff using manual defibrillators is a standard of care that underpins modern cardiac intensive care.
Speed, Automation, and Accessibility
Modern defibrillators are engineered for speed and ease of use. AEDs can be ready to deliver a shock within 8–15 seconds of being powered on, providing rapid charging and automated analysis that removes the diagnostic burden from untrained bystanders. The step-by-step voice and visual prompts of AEDs enable individuals with no medical training to deliver potentially life-saving shocks in public settings. AEDs have been demonstrated to be safe and effective when used by children as young as 9–10 years old, supporting widespread placement in schools. For ICD patients, continuous 24/7 autonomous monitoring eliminates the risk of missing a fatal arrhythmia event during sleep or other vulnerable periods.
Integration with Monitoring Ecosystem
Contemporary defibrillators integrate seamlessly with patient monitoring ecosystems, transmitting real-time ECG data to hospital information systems, cardiac catheterization labs, and remote monitoring platforms. The integration of defibrillator data with electronic health records (EHRs) supports post-event analysis, quality improvement, and protocol compliance auditing. Dual-function monitor-defibrillators, common in emergency departments and intensive care units, combine the capabilities of a full-featured cardiac monitor with manual defibrillation, synchronized cardioversion, and external pacing in a single portable device. This multifunctionality reduces equipment overhead and ensures continuous rhythm surveillance throughout resuscitation and post-resuscitation care.
7. What are general risks or limitations?
Myocardial Damage and Tissue Injury
Despite advances in biphasic waveform technology, defibrillator shocks carry inherent risks of cardiac and non-cardiac tissue injury. Excessive delivered energy can cause direct myocardial damage, manifested as transient ST-segment elevation, elevated cardiac biomarkers (troponin), post-shock cardiac dysfunction, and in extreme cases, frank myocardial necrosis. Skin burns at electrode sites remain a concern, particularly with repeated shocks, inadequate electrode contact, or use of inappropriate electrode gel. Cumulative shock energy delivered during prolonged resuscitation must be monitored to balance therapeutic benefit against tissue injury. Biomedical engineers working on device design must carefully optimize waveform parameters to maintain efficacy while minimizing energy deposition at both the electrode-skin interface and within the myocardium itself.
Inappropriate Shocks and Algorithm Limitations
A significant complication of ICD therapy is the delivery of inappropriate shocks — shocks triggered by non-life-threatening arrhythmias such as rapid atrial fibrillation, sinus tachycardia, or electrical noise from lead fractures or electromagnetic interference. Inappropriate ICD shocks cause significant patient distress, impair quality of life, and are associated with increased mortality risk, potentially due to their proarrhythmic effects and psychological consequences including anxiety and depression. Reported rates of inappropriate shocks in legacy ICD systems have historically ranged from 10–20% of patients over multi-year follow-up. Rhythm discrimination algorithms, dual-coil lead configurations, and remote monitoring have progressively reduced inappropriate shock rates, but they remain a meaningful clinical challenge driving ongoing R&D investment.
Non-Shockable Rhythms and Operator Limitations
A critically important limitation of defibrillators is that they are effective only for shockable rhythms — VF and pVT. Non-shockable rhythms such as asystole (flatline) and pulseless electrical activity (PEA) do not benefit from defibrillation; these conditions require identification and treatment of underlying reversible causes (the “Hs and Ts” of ACLS), CPR, and pharmacological intervention. Misidentification of rhythm type by untrained users or, in rare cases, algorithmic failure in AEDs, can result in unnecessary or missed shocks. Additionally, motion artifact during CPR can interfere with AED rhythm analysis, causing unnecessary pauses in compressions. Operator error — including incorrect electrode placement, failure to maintain device readiness, and insufficient CPR quality — remains a significant contributor to poor outcomes despite best device design.
8. How is the Defibrillator evolving / recent innovations?
Artificial Intelligence and Advanced Rhythm Analysis
One of the most transformative developments in defibrillator technology is the integration of artificial intelligence (AI) and machine learning (ML) algorithms for cardiac rhythm analysis. AI-based rhythm detection systems trained on large annotated ECG databases can distinguish VF from non-shockable rhythms with higher sensitivity and specificity than traditional threshold-based algorithms, particularly in the presence of motion artifacts (such as during active CPR compressions). ZOLL Medical’s CPR-D algorithm and similar implementations from other manufacturers have demonstrated the ability to analyze rhythm during uninterrupted chest compressions, potentially eliminating the need for CPR pauses for rhythm checks. AI is also being applied to ICD therapy optimization, reducing inappropriate shocks by more accurately distinguishing supraventricular from ventricular tachycardias using multi-feature morphology analysis.
Implantable and Leadless Device Innovations
The subcutaneous ICD (S-ICD), pioneered by Cameron Health and now commercialized by Boston Scientific, has gained widespread adoption due to its avoidance of intravascular leads. The entirely extravascular shock vector delivers effective defibrillation at energies up to 80 J without any leads inside the heart or vasculature, dramatically reducing the risk of lead-related infections, thrombosis, and vascular injury. The Medtronic Micra™ Transcatheter Pacing System, the world’s first commercially available leadless pacemaker, has inspired development toward leadless ICD platforms, with early-stage devices such as the EV-ICD (extravascular ICD) system currently in clinical trials. Miniaturization through advanced battery chemistry, including solid-state lithium batteries, is enabling smaller device profiles and longer service lives (10–15 years) for next-generation implantables.
Wearable Technology and Telehealth Integration
Wearable cardioverter-defibrillators (WCDs), such as the ZOLL LifeVest™, have expanded the protective reach of defibrillation therapy to outpatients at high but potentially transient risk of SCA — including patients recovering from myocardial infarction, those with newly diagnosed cardiomyopathy, or post-cardiac surgery patients awaiting ICD implantation. Next-generation WCDs integrate continuous multi-lead ECG monitoring, accelerometers for activity tracking, and cellular connectivity for real-time data transmission to cardiologists and remote monitoring centers. Telehealth platforms allow physicians to review daily arrhythmia summaries, receive automated alerts for significant events, and adjust device parameters remotely. This convergence of defibrillation capability with telehealth infrastructure represents a fundamental shift in how high-risk cardiac patients are managed outside of hospital walls, and aligns with broader trends in digital health and remote patient monitoring.
9. Key takeaways / tips for biomedical engineers
Design, Testing, and Regulatory Compliance
Biomedical engineers designing or evaluating defibrillators must have a thorough understanding of the governing standards. The primary standard for cardiac defibrillators is IEC 60601-2-4, which specifies safety and performance requirements including delivered energy accuracy (±15%), waveform characteristics, defibrillation algorithm testing protocols, and electromagnetic compatibility. This standard works in conjunction with IEC 60601-1 for general electrical safety and medical electrical equipment requirements. In the United States, defibrillators are Class III medical devices regulated under FDA 21 CFR Part 870 (cardiovascular devices), requiring either a 510(k) clearance or PMA (Premarket Approval) for new devices. Manufacturers must maintain a quality management system compliant with ISO 13485. Engineers should also be familiar with AHA/ERC (European Resuscitation Council) resuscitation guidelines, which drive clinical performance benchmarks that device algorithm performance must meet or exceed.
Maintenance, Verification, and Safety Engineering
From a clinical engineering and biomedical equipment management perspective, maintaining defibrillator readiness is a non-negotiable safety requirement. Key maintenance activities include: regular delivered-energy verification using a calibrated defibrillator analyzer (e.g., Fluke Biomedical), electrode pad expiration date checks, battery capacity testing, and self-test log review. AEDs in public access programs require a structured inspection and maintenance schedule to ensure they are functional when needed. Engineers should understand the capacitor aging phenomenon — capacitors in defibrillators are subject to charge-discharge cycling wear and dielectric degradation, requiring periodic replacement per manufacturer specifications. Failure mode and effects analysis (FMEA) and fault tree analysis (FTA) are critical tools in the design verification process to identify and mitigate potential failure modes before market release.
Emerging Research Areas and Career Opportunities
For biomedical engineers looking to contribute to defibrillator innovation, several high-value research areas present significant opportunities. Waveform optimization research — particularly adapting delivered waveform parameters in real time based on patient impedance feedback — continues to be an active area with measurable clinical impact. AI algorithm development for rhythm classification, especially during active CPR, is one of the fastest-growing domains combining clinical electrophysiology with data science. Battery and power electronics miniaturization for next-generation ICDs and WCDs requires expertise in electrochemistry and high-density energy storage. Finally, the development of fully leadless, wirelessly communicating implantable defibrillation systems represents perhaps the most ambitious long-term engineering challenge in the field. As defibrillators become more connected, cybersecurity for implantable and networked devices has emerged as a critical discipline — one that requires cross-disciplinary expertise spanning hardware security, regulatory affairs, and clinical safety. Familiarity with the broader cardiac monitoring ecosystem, including ECG machines and ambulatory monitoring technologies, is an important foundation for any engineer specializing in electrocardiology devices.
References
- Zipes DP, et al. “ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death.” Journal of the American College of Cardiology, 48(5), 2006.
- Cobb LA, et al. “Changing Incidence of Out-of-Hospital Ventricular Fibrillation, 1980–2000.” JAMA, 288(23):3008–3013, 2002.
- IEC 60601-2-4:2010+AMD1:2020. Medical Electrical Equipment – Part 2-4: Particular Requirements for the Basic Safety and Essential Performance of Cardiac Defibrillators. International Electrotechnical Commission.
- Lown B, et al. “The Electrical Conversion of Cardiac Arrhythmias.” British Heart Journal, 29(4):469–489, 1967.
- Bardy GH, et al. “A Simplified, Single-Lead Unipolar Transvenous Cardioversion-Defibrillation System.” Journal of the American College of Cardiology, 22(1):96, 1993.
- Priori SG, et al. “2015 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death.” European Heart Journal, 36(41):2793–2867, 2015.
- US Food and Drug Administration. “Guidance for Industry and FDA Staff: Cardiac Defibrillators — Premarket Notification [510(k)] Submissions.” FDA, 21 CFR Part 870.
- Jacoby JL and Cohn BG. “Defibrillation.” In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 2024.
- Abd-Alkhalek, N. H., Khuter, H. T. Y., Hadi, R. T. A., Abdel, H. H. A., & Khreeb, M. M. A. (Eds.). (2025). Defibrillators: Principles, design, and clinical applications (1st ed.). Bright Sky Publications. https://doi.org/10.62906/bs.book.414
